
This 53 year old man is an ex-smoker, with HTN well controlled by a single agent.
He presented to the ED under duress from his wife and GP with intermittent atypical pain which is sometimes worse with exertion, has a slight pleuritic variation, and radiates to shoulders. He mentions a more severe pain 2 days ago lasting a couple of hours with onset at rest. This was preceded by about three weeks of occasional slight exertional dyspnoea and chest tightness.
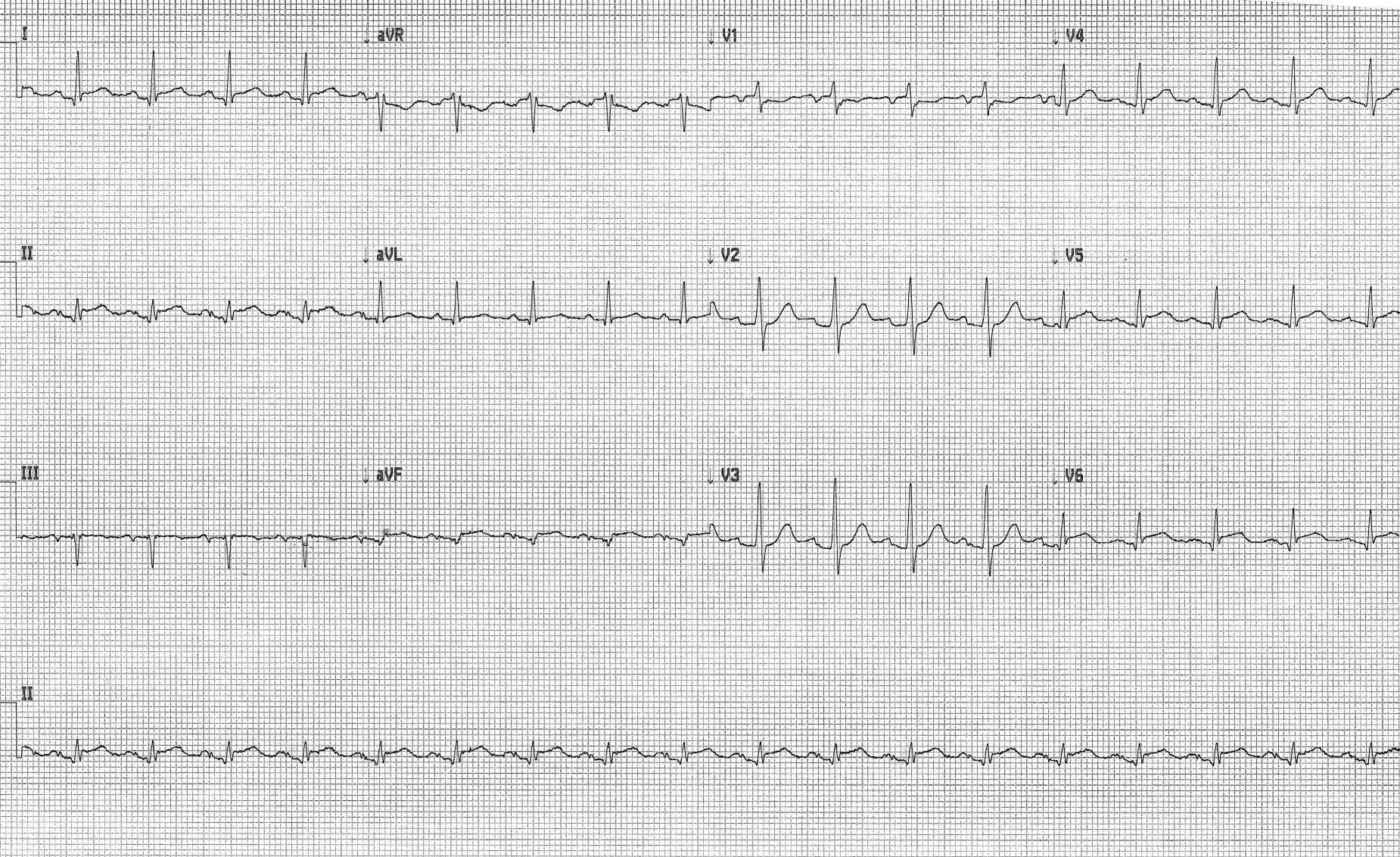
This is his ECG with mild residual discomfort:
What are your thoughts?


there is left atrial abnormality and pericarditis
so ??? its in the inferior leads ??
Posterior MI
PR-elevation and ST-depression in aVR lead me to believe pericarditis.
Reblogged this on the underneaths of EM and commented:
There is ST elevation in I, II and aVF (i.e. missing out III) and V5 and V6 (and a hint in V4). There is apparent ST depression in aVR, but as some of you point out, this actually represents PR elevation. Of note, III is NOT elevated, which makes an inferolateral STEMI pretty unlikely. One might also expect some ST segment depression in aVL, and clearly there is none. As mentioned in one comment, there is likely to be left atrial abnormality with an asymmetrically bifid P-wave most marked in II. The first TnT was 16….now what? Do you activate the cath lab? Is it clearly pericarditis, or could it be STEMI?
There is ST elevation in I, II and aVF (i.e. missing out III) and V5 and V6 (and a hint in V4). There is apparent ST depression in aVR, but as some of you point out, this actually represents PR elevation. Of note, III is NOT elevated, which makes an inferolateral STEMI pretty unlikely. One might also expect some ST segment depression in aVL, and clearly there is none. As mentioned in one comment, there is likely to be left atrial abnormality with an asymmetrically bifid P-wave most marked in II. The first TnT was 16, and he still has a niggle of pain….now what? Do you activate the cath lab? Is it clearly pericarditis, or could it be STEMI? Give me a plan…
mild left ventricular hypertrophy secondary to an old lateral (circumflex) injury
STEMI seems unlikely given the above. How long has his pain been going this time? If this atypical niggling pain represents a STEMI and has been going on for several hours I would expect development of q waves – none clearly pathological although low voltage in inferior leads. As mentioned there is no reciprocal ST depression. The widespread ST elevation with PR depression and then PR elevation in aVR is much more suggestive of a pericarditis. Not familiar with TnT but if similar to TnI a level of 16 would be suggestive of a myopericarditis.
As a few people have mentioned on twitter, discussion with interventional cardiologist would be key. Admit CCU, get echo, serial ECGs. Reconsider if serial ECGs demonstrate more of an ischaemic pattern. Aspirin but would be nervous about anticoagulation.
Pingback: Not all ST elevation is STEMI – the follow up | the underneaths of EM
Pingback: Previous Post | the underneaths of EM